What is Everolimus (159351-69-6) used for?
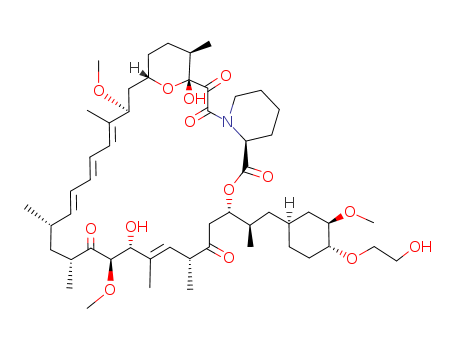
Everolimus, an oral immunosuppressant for the treatment of kidney and heart
transplant rejection, is the 40-O-(2-hydroxyethyl) derivative of rapamycin. It has
immunosuppressive properties similar to those of rapamycin, but with improved
pharmacokinetic profile. In addition, the 40-O-(2-hydroxyethyl) group alters
the physico-chemical properties of the macrolide to allow galenic formulation.
Everolimus is prepared in a two-step semisynthesis starting from rapamycin,
by alkylation of the 40-hydroxyl group with t-butyldimethylsilyloxyethyl triflate
and subsequent cleavage of the silyl protecting group. Everolimus, like rapamycin,
is a proliferation signal inhibitor that exerts its immunosuppressive effect by inhibiting
the activation of p70 S6 kinase, thereby blocking growth factor-driven
proliferation of T cells, B cells and vascular smooth muscle cells, and arresting
cell cycle at the G1 phase. Inhibition of p70 S6 kinase activation by everolimus and
rapamycin is mediated by their binding to FKBP12 (FK506 binding-protein
12). Everolimus inhibits FK506 binding to FKBP12 with an IC50 of 1.8–2.6 nM,
and it is about 3- to 5-fold less potent than rapamycin (IC50=0.4–0.9 nM). The
in vitro immunosuppressive activity of everolimus is also slightly less than that
of rapamycin as demonstrated in a mixed lymphocyte reaction (MLR) assay
(IC50=0.2–1.6 nM versus 0.07–0.5 nM, respectively) and in antigen-specific
human helper T-cell clones (IC50=0.05–0.17nM versus 0.014–0.37nM, respectively).
However, the in vivo immunosuppressive activity of oral everolimus 1–5 mg/
kg/day is similar to that of rapamycin at equivalent doses in rat models of renal or
cardiac transplantation, localized graft-versus-host disease, and autoimmune
glomerulonephritis. The recommended dosage of everolimus is 0.75 mg twice
daily, and it is used in combination with cyclosporine microemulsion and corticosteroids.
Following oral dosing, the peak concentration (Cmax) of everolimus
is estimated between 1.5 to 2 hours, and steady state is achieved within 4 days.
The terminal elimination half-life is 21 to 35 hours. By comparison, rapamycin has
a longer elimination half-life (60 hours) and longer time to reach steady state (7 to
14 days). Consequently, rapamycin treatment requires a large loading dose, followed
by once daily maintenance dose, whereas everolimus is administered twice
daily but without the need of a loading dose. Everolimus is extensively metabolized,
primarily by CYP3A4. Approximately 80% of the dose is excreted in the feces and
about 5% in the urine. In clinical trials with adult cardiac transplant recipients, oral
everolimus 0.75 or 1.5 mg twice daily significantly reduced the incidence of efficacy
failure as well as cardiac allograft vasculopathy (CAV) up to 2 years after transplantation
as compared with azathioprene 1–3 mg/kg/day. However, graft and patient
survival rates at 1 year were similar in patients receiving everolimus and
azathioprene. In trials involving renal transplant recipients, the combined incidence
of biopsy-confirmed acute rejection, graft loss, death, or loss to follow-up was
similar in patients receiving everolimus 1.5 or 3 mg/day or mycophenolate mofetil 2
g/day up to 3 years after transplantation. Everolimus was well tolerated in transplant
patients. The incidence of viral infection including cytomegalovirus (CMV)
was reduced in comparison to azathioprene and mycophenolate mofetil, but bacterial
infections were more frequent. Main adverse events associated with everolimus
were thrombocytopenia, leucopenia, and elevated serum lipids and
creatinine.
InChI:InChI=1/C53H83NO14/c1-32-16-12-11-13-17-33(2)44(63-8)30-40-21-19-38(7)53(62,68-40)50(59)51(60)54-23-15-14-18-41(54)52(61)67-45(35(4)28-39-20-22-43(66-25-24-55)46(29-39)64-9)31-42(56)34(3)27-37(6)48(58)49(65-10)47(57)36(5)26-32/h11-13,16-17,27,32,34-36,38-41,43-46,48-49,55,58,62H,14-15,18-26,28-31H2,1-10H3/b13-11-,16-12+,33-17+,37-27-/t32-,34-,35-,36-,38-,39+,40+,41+,43-,44+,45+,46-,48-,49+,53-/m1/s1
Articles related to Everolimus: